
What is ribosome synthesis?
Congenital ribosomopathy
Hallmarks of ribosompathies
References
Further reading
Defects in ribosome biogenesis, assembly, and function of individual ribosomes are termed ribosomopathies. They are characterized by tissue-specific phenotypic abnormalities that consequently increase cancer risk in later life. The discovery of ribosomal mutations in ribosomal proteins (RPs) and defects in ribosomal structure among several types of tumors have reinforced their association with cancer.
The definition of ribosomopathies may also be extended to include some cancers with somatic ribosomal protein gene mutations, as these mutations are implicated in direct causality.
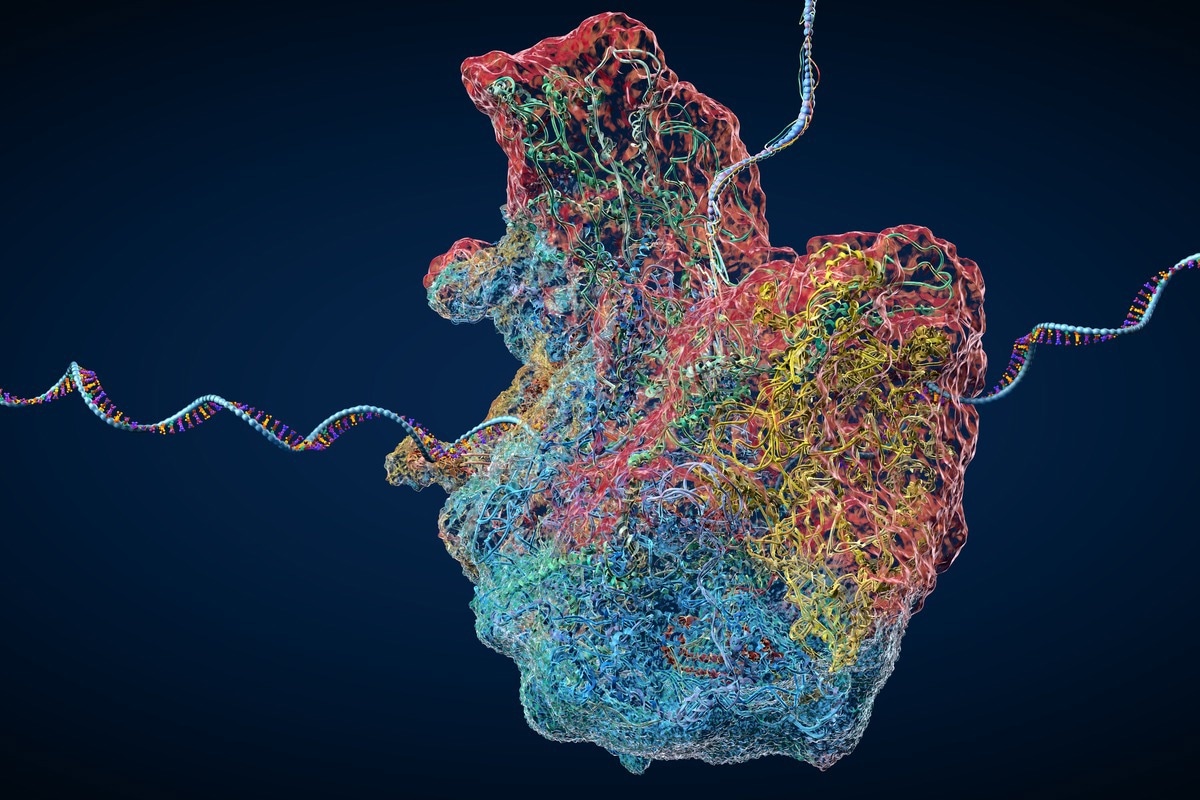
Image Credit: Christoph Burgstedt/Shutterstock.com
In some instances, cancers may arise from multiple genetic mutations, including somatic ribosomal protein mutations. A somatic ribosomal protein mutation can therefore promote the transformation of cancer but will not be sufficient on its own to cause it. They and mutations in ribosome biogenesis factors can cause the hyperproliferative phenotypes seen in early congenital ribosomopathy. Therefore, ribosomopathies can be classified into somatic and congenital.
What is ribosome synthesis?
Ribosome synthesis is an essential, energy-demanding process that involves the coordination of 200 accessory factors and 80 ribosomal proteins (r-proteins) to produce and assemble mature ribosomal proteins (rRNAs)
Most ribosome biogenesis occurs in the nucleolus, beginning with the transcription of 47S pre-rRNA from ribosomal DNA loci by the enzyme RNA Polymerase I (RNAPI). After this, the pre-RNA is processed to yield 18S, 5.8S, and 28S, representing three of the four requisites of mature rRNAs. This rRNA is modified by small nucleolar ribonucleoproteins (snoRNPs), subsequently assembled with r-proteins. The fourth rRNA is transcribed by RNAP III from a locus outside the nucleolus. These steps produce the mature small subunit SSU, or 40S, and the 60S large subunit, LSU.
These come together in the cytoplasm to produce a functioning ribosome that can translate messenger RNA and mRNA. The improper synthesis of ribosomes is subsequently associated with several disorders, for example, bone marrow failure syndrome and Diamond Blackfan Anemia (DBA). Since their discovery, new ribosomopathies have been discovered, which are expressed in a tissue-specific manner.
Therefore, a defect in any one of the components of the essential ribosomal apparatus is associated with impaired cellular function. As mentioned, a hallmark of these disorders is their highly sensitive manifestation, which occurs in a tissue-specific manner to exert a tissue-specific phenotype.
Congenital ribosomopathy
Mutations implicated in ribosomopathies were first discovered in 1999 in patients with congenital bone marrow failure syndrome, DBA. This congenital ribosomopathy is characterized by early-life bone marrow failure manifestations and subsequent increased risk of cancer development in later life. Since this discovery, ribosomal protein mutations have been identified in approximately half of all DBA patients, specifically with loss of function mutations found at the highest frequencies in the ribosomal proteins RPS19, RPL5 (uL18), RPL11 (uL5), and RPS10 (eS10).
A list of other congenital syndromes has been linked to defects in the biogenesis factors, each of which change is a specific step in the biogenesis process. Alongside DBA, the most studied ribosomopathies are:
- Shwachman-Diamond syndrome (SDS): most patients display an activating mutation in the SBDS gene, which encodes a factor involved in the maturation of the 60S subunits. Normally the factor EIF6 keeps the nascent 60S subunit inactive during its assembly to prevent it from prematurely associating with the 40S subunit; SBDS promotes the release of this factor, and as a result of its activation, the release of EIF6 does not occur, which stores this maturation of 60 S. This congenital ribosomopathy is characterized by early-life bone marrow failure manifestations and subsequent increased risk of cancer development in later life.
- X-linked dyskeratosis congenital (DC): 25% of patients with DC carry mutations in the DKC1 gene, which encodes an enzyme that causes pseudouridylation of rRNA. It also plays a role in the maintenance of telomeres; in DC, there are also associated mutations in telomerase genes such as TINF2, TERC, or TERT. This congenital ribosomopathy is characterized by early-life bone marrow failure manifestations and subsequent increased risk of cancer development in later life.
- Cartilage hair hypoplasia (CHH : This is caused by mutated RMRP, a component of the RNAse mitochondrial RNA processing complex. Mutations in this gene prevent rRNA processing by preventing its cleavage, which prevents the maturation of the 18S and 5.8S rRNA
- Treacher Collins syndrome (TCS): this congenital ribosomopathy is not associated with an increased risk of cancer in later life. Relative to other defects in ribosomal proteins that are connected to specialized translation of a subset of genes that control hematopoiesis, TCS does not share this property. It is caused by a lack of polymerase I/III, which reduces the production of mature ribosomes and lowers the translation rate, resulting in weakened cells that promote a quiescent/ inactive state.
Somatic ribosomopathies are several mutations in the ribosomal protein genes associated with somatic ribosomeopathies. Some somatic mutations and deletions are more strongly proportional to the incidence of the cancer type.
Image Credit: Rost9/Shutterstock.com
RLP5 is strongly associated with incidents of breast cancer, and it is thought to play a tumor suppressor role in the context of breast cancer. In contrast, the loss of RLP5 prevents the proliferation of normal cells. Heterozygous loss of RPL5 by deletions or inactivating mutations occurs in 2% of T-ALL samples and up to 30% of multiple myeloma, melanoma, glioblastoma, and breast cancers.
RLP22 is implicated in T-ALL, (4%) and ~10% of endometrial, colorectal, and gastric cancer samples. RLP23A is found in 12.5% of uterine cancers. RPS15 is seen in 20% of patients with relapsed chronic lymphoid leukemia (CLL).
Hallmarks of ribosompathies
Ribosomopathies are caused by a collection of phenotypic manifestations. In summary, ribosomopathy ‘lesions,’ that is, mutations that affect the function of ribosome biogenesis and ribosomal proteins affect the translation of hematopoietic and cancer-promoting mRNAs. Subsequently, proteasome function is altered, which can either stabilize or increase the degradation rate of subsets of proteins, including oncogenes and tumor suppressors.
In addition, ribosomopathies show rewiring of the metabolism; this reprogramming of specific subsets of proteins that support the alternative metabolic requirements of the ribosomal protein defective cells is not known (known as specialized translation).
These cells affected by ribosomopathies also demonstrate increased levels of oxidative DNA damage that can cause secondary mutations to be acquired, which have a key function in transforming cells into cancerous cells. In addition, the extra ribosomal function of mutated ribosomal proteins can be influenced by lesions.
Since their discovery over 20 years ago, a large deal of progress has been made in understanding ribosompathies. Most notably, these findings have promoted novel therapeutic approaches being explored preclinically or implemented in the clinical setting. Despite these advances, several questions remain. There is an unknown understanding of ribosome specialization, particularly because in both somatic and congenital ribosomopathy, a differential translational output of ribosomes occurs.
A second question is the spectrum of mutations associated with ribosompathies. In many subsets of some congenital ribosompathies, the causal mutation is unknown, and in somatic ribosompathies, the genes implicated in ribosomopathies are also known to have other functions. Therefore, this confounds the understanding of how genes promote cancer.
References
- Kampen KR, Sulima SO, Vereecke S, et al. (2020) Hallmarks of ribosomopathies. Nucleic Acids Res. doi: 10.1093/nar/gkz637.
- Farley-Barnes KI, Ogawa LM, Baserga SJ. (2019) Ribosomopathies: Old Concepts, New Controversies. Trends Genet. doi:10.1016/j.tig.2019.07.004.
Last Updated: Jun 23, 2022

Written by
Hidaya Aliouche
Hidaya is a science communications enthusiast who has recently graduated and is embarking on a career in the science and medical copywriting. She has a B.Sc. in Biochemistry from The University of Manchester. She is passionate about writing and is particularly interested in microbiology, immunology, and biochemistry.
Source: Read Full Article