
Researchers have conducted a study showing that the B.1.1.7 variant of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that has emerged in the UK is associated with a significantly increased risk of death compared with the viral strain previously circulating in the country.
The SARS-CoV-2 virus is the agent responsible for the coronavirus disease 2019 (COVID-19) pandemic that has now caused more than 117 million infections and claimed more than 2.6 million lives worldwide.
The team’s study of an unvaccinated population found that the B.1.1.7 variant of concern (VoC) was associated with a two-thirds higher case fatality rate, compared with the strain previously circulating in this population. The risk of death was higher among males than females and increased with age and the number of comorbidities.
The B.1.1.7 variant has become the dominant SARS-CoV-2 strain in the UK and is now increasing in prevalence across Europe.
Daniel Grint from the London School of Hygiene & Tropical Medicine and colleagues warn that policy planners need to account for the higher mortality rate associated with this VoC.
They also say the study highlights the importance of robust national vaccination programs and infection control measures to contain the spread of SARS-CoV-2.
Uncontrolled spread of the B.1.1.7 variant could be faster and more deadly than has so far been seen during the pandemic, warns the team.
A pre-print version of the research paper is available on the medRxiv* server, while the article undergoes peer review.
.jpg)
B.1.1.7 variant likely to become dominant across Europe
The B.1.1.7 variant, which was first identified in the UK in autumn 2020, is now likely to become the most common strain of SARS-CoV-2 across Europe.
Early studies suggested that this VoC is more transmissible than previously circulating strains and is associated with increased mortality.
However, previous reports of increased mortality did not include data on individuals’ comorbidities, says Grint and the team.
“Accurate estimation of disease severity associated with this VoC is critical for pandemic planning,” they write.
What did the researchers do?
Working on behalf of NHS England, the team drew data from the OpenSAFELY electronic health records (EHR) secure research platform, which covers 40% of the population in England registered with a general practitioner (GP).
Linked GP, SARS-CoV-2 testing, vaccination and mortality data were used to estimate fatality risk following diagnosis of SARS-CoV-2 infection with the B.1.1.7 variant versus non-VoC strains between 16th November 2020 and 11th January 2021.
Infection cases were followed up until 5th February 2021 or seven days prior to receiving a SARS-CoV-2 vaccine, whichever came first.
What did the study find?
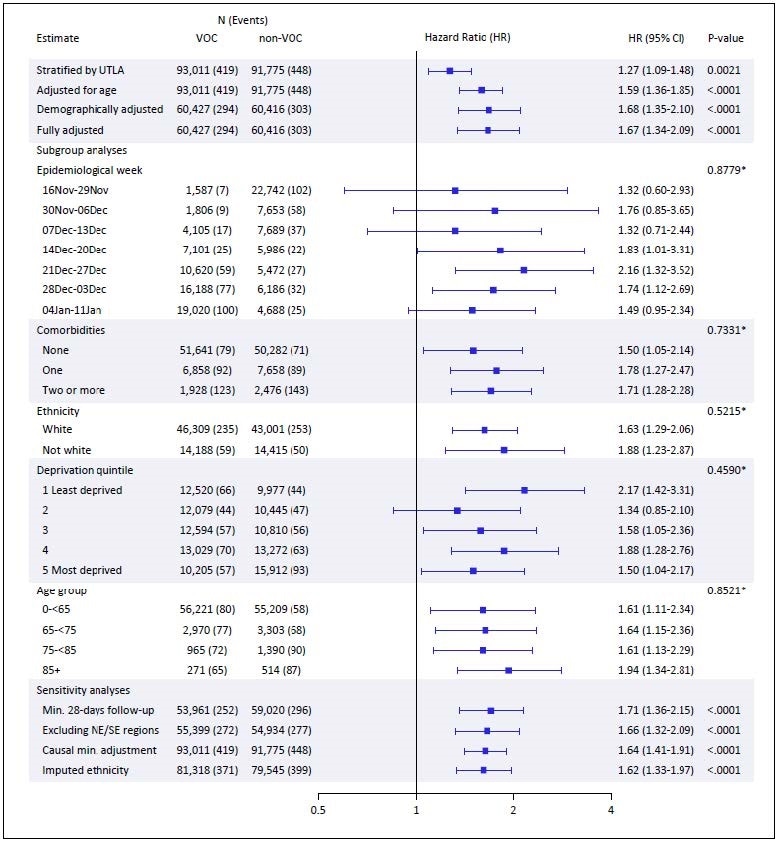
Cox regression analysis revealed that infection with the B.1.1.7 variant was associated with a 67% increased risk of death, compared with non-VoC infections, after full adjustment for demographics and comorbidities.
Analysis of the absolute risk of death within 28 days of testing positive for SARS-CoV-2 found that infection with the VoC was associated with a 73% increased likelihood of death, compared with non-VoC infection.
The 28-day risk of death was low for those aged under 65 years without comorbidities, although it was higher for males than females.
The risk of death by day 28 among males and females in this group was 0.14% and 0.07%, respectively, for VoC infection, compared with 0.09% and 0.05%, respectively, for non-VoC infection.
The risk of death was consistently higher for males and increased with age and the number of comorbidities.
The highest risk was observed for those aged 85 and older with two or more comorbidities. The risk of death among males and females in this group was 24.3% and 14.7%, respectively, for VoC infection, compared with 16.7% and 9.7%, respectively, for non-VoC infection.
The B.1.1.7 VoC has the potential to spread faster and be more deadly
“We find this VoC is associated with two-thirds higher case fatality than the previously circulating virus in this unvaccinated population,” writes Grint and colleagues.
“Unmitigated spread of this VOC has the potential to be both faster and more deadly than has been seen in the pandemic to date,” they warn.
The researchers say that, crucially, emerging data suggest that the currently approved vaccines against SARS-CoV-2 are effective against the B.1.1.7 variant.
“This study highlights the importance of robust national vaccination programs and infection control measures to contain the SARS-CoV-2 pandemic,” concludes the team.
*Important Notice
medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
- Grint D, et al. Case fatality risk of the SARS-CoV-2 variant of concern B.1.1.7 in England. medRxiv, 2021. doi: https://doi.org/10.1101/2021.03.04.21252528, https://www.medrxiv.org/content/10.1101/2021.03.04.21252528v1
Posted in: Medical Research News | Disease/Infection News
Tags: Coronavirus, Coronavirus Disease COVID-19, General Practitioner, Hygiene, Infection Control, Medicine, Mortality, Obesity, Pandemic, Research, Respiratory, SARS, SARS-CoV-2, Severe Acute Respiratory, Severe Acute Respiratory Syndrome, Smoking, Syndrome, Vaccine, Virus

Written by
Sally Robertson
Sally first developed an interest in medical communications when she took on the role of Journal Development Editor for BioMed Central (BMC), after having graduated with a degree in biomedical science from Greenwich University.
Source: Read Full Article