. DOI: 10.1371/journal.pone.0274703")
In 2012, Michael Cruz exercised a lot. Four years into a 15-year prison sentence, this was one of the only things he had, he says, until he noticed a numb, tingling sensation in one of his toes while working out. At first, he dismissed the feeling. But it persisted, and over time, spread up his ankle. Then, he began experiencing little sharp pains in his back, which he attributed to muscle spasms from his workouts. Months later, the tingling sensation had encompassed his body up to his belly button. And when he woke up one morning, legs shaking and unable to walk, he knew he needed to see a doctor.
That year, he was diagnosed with non-Hodgkin’s lymphoma. Initial signs of the cancer can often include swollen lymph nodes, weight loss, and fever. But for Cruz, if it weren’t for a tumor on his spine pushing against his nerves, creating the strange tingling, he would not have known about the deadly disease spreading inside him.
“I was 42 years old, working out, healthy, jogging, and playing sports,” he says. “I never really put thought into [getting sick.] Then my whole life changed.”
Since his initial diagnosis, he has undergone numerous chemotherapy and radiation treatments, surgeries, biopsies, and PET and CAT scans. He lost weight, hair, and his appetite.
Despite the efforts of his medical team, his cancer returned in 2014 and again at the end of 2017. In 2020, he was granted a compassionate release, and is continuing to receive treatment.
Cancer is a harrowing journey for anyone, but for incarcerated and formerly incarcerated patients like Cruz, receiving care for the life-altering disease presents extra challenges. The United States has one of the highest incarceration rates in the world, with nearly 2 million people in the criminal justice system facing potential barriers to accessing timely, quality care.
Now, research led by Emily Wang, MD, professor of medicine (general medicine) and of public health (social and behavioral sciences) and director of the SEICHE Center for Health and Justice; and Cary Gross, MD, professor of medicine (general medicine) and of epidemiology (chronic diseases) and founder and director of the Cancer Outcomes, Public Policy, and Effectiveness Research (COPPER) Center, seeks to understand the public health ramifications of mass incarceration in the U.S. They are finding that individuals with a history of incarceration are more likely to be diagnosed with cancer and are less likely to survive the disease. The findings are published in the journal PLOS ONE.
“After leaving prison, formerly incarcerated persons have higher health risks than people in the general population,” says Gross. “Given the very high prevalence of incarceration in this country, this becomes a public health issue.”
Lifelong consequences of mass incarceration disproportionately affect people of color
The U.S. has a “shockingly high” incarceration rate, says Gross. He and Wang believe this is a result of oppressive systems and policies including the war on drugs, a fractured mental health care system, and an inadequate social safety net system. And the consequences of mass incarceration continue to haunt the 70 to 100 million Americans with criminal records long after they complete their sentences. “These are called collateral consequences,” says Wang. “They prevent people who have been incarcerated or have criminal records from getting social needs met through either legal or policy barriers to obtaining employment, housing, and food.”
Furthermore, they argue incarceration perpetuates centuries of racial oppression. Young Black men are disproportionately at greatest risk for incarceration. In 2020, for example, Black adults were incarcerated at a rate nearly five times greater than white adults. And while Black youth make up only 15% of the U.S. population under 18, they account for 35% of youth arrested.
The health impact of incarceration
Research has demonstrated the troubling health impacts of incarceration. A study led by Wang as first author and senior author Harlan Krumholz, MD, Harold H. Hines, Jr. Professor of Medicine (Cardiology), found that individuals just released from incarceration are hospitalized at a substantially higher rate than the general population—around one in 70 people are hospitalized within seven days of release, and one in 12 by 90 days. In 2019, a study led by Wang and Gross found that those with prior criminal justice involvement were substantially more likely to be diagnosed with certain cancers, including lung and cervical cancers.
“We spend so much money on health care for the incarcerated, but the perverse public health impacts of incarceration on families and communities are unexplored and underappreciated,” says Wang. “It’s something we almost never learned about in medical school, and I suspect most oncologists don’t think explicitly about the care of incarcerated patients.”
Before joining forces, Wang and Gross had offices next door to each other for many years. “Our collaboration is really a testament to our amazing environment here at Yale,” says Gross. “Emily has a long-standing interest in the impact of incarceration and health. I have a long-standing interest in cancer, cancer equity, and cancer outcomes. And we eventually realized that our two interests could easily overlap.” The two decided to come together and are now researching the links between incarceration and cancer incidence and cancer mortality.
Greater risk of cancer diagnosis soon after release
Research estimating cancer incidence in individuals during and post-incarceration is lacking due to the numerous challenges this work poses. National surveys and claims data often fail to include incarceration status. Furthermore, care for these individuals is often fragmented, making it difficult to track cancer diagnosis and treatment.
Thus, Wang and Gross’s team sought to compare the cancer incidence in incarcerated and post-incarcerated individuals with that of the general population in Connecticut, as well as specifically look at the incidence in Black individuals. First, they used data from the Connecticut Tumor Registry and Connecticut Department of Corrections to identify all cancer diagnoses between 2005 and 2016. For patients involved with the criminal justice system, the team noted whether the diagnosis occurred during incarceration or post-release.
Their work revealed that cancer was detected at a significantly lower rate among incarcerated individuals compared to the general population. On the other hand, the team found a significantly higher rate of cancer incidence among individuals who were recently released from prison. “As our next step, our team is working to find why this occurs,” says Wang. “Is there a pent-up demand for screening or evaluation of symptoms among people who are incarcerated?” One thought is that this may be a product of lack of access to consistent screening.
Furthermore, regardless of incarceration status, the study found that Black individuals faced a greater risk of being diagnosed with a screen-detectable cancer than white individuals.
Health problems of incarcerated people may be ignored
Getting medical help while in prison can be challenging, Cruz confirms. He feels grateful that the woman he pulled aside listened to him and got him help right away. “If I went to a different person, I don’t think I would have gone to the hospital that same day,” he says. “Sometimes it take weeks [to get help], sometimes it takes months. And those weeks and months could be life-changing for somebody.”
He recalls watching several of his fellow inmates complain about being in pain but having to wait months or even a year for help. For cancer patients, these delays in being diagnosed or accessing care may be deadly. “Let’s say you’re in a facility dealing with over 3,500 inmates and 3,000 are crying wolf. But there are still 500 that have a real medical condition,” he says. “A lot of correctional officers have lost the compassion and humility to take the time to see if there’s something wrong with you, because they’ve just dealt with 1,000 people who just said they were sick so they could leave their cell. And here you are actually sick, but you are 1,001.”
While he thinks that that his cancer was diagnosed and treated relatively quickly, Cruz says other incarcerated cancer patients were not as lucky. He recalls a time in which he stayed in an infirmary with 10 other patients, and only three walked out. “I would be talking to somebody and could smell the death coming out of them,” he says. “It smelled like their body was decaying on the inside.”
It can be especially difficult, he continues, if patients don’t have a support system. “[Getting timely care] is a big problem, especially if you don’t have someone to help give you a voice,” he says. “I’m grateful that I had my daughter—if something was wrong, she’d call the facility. Once they see that you have outside family, they tend to take care of you more quickly as opposed to those just speaking for themselves.”
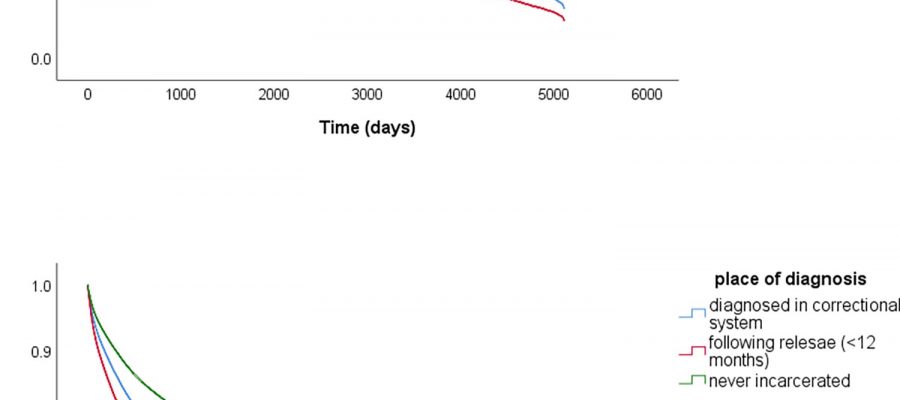
Beyond facing a greater cancer risk, incarcerated and formerly incarcerated individuals also face higher rates of mortality due to the disease, Wang and Gross’s team found in the recently published study among 216,540 adults diagnosed with an invasive cancer in Connecticut. Their work identified the first 12 months post-release as an especially high-risk period time in terms of survival. It also found that incarcerated individuals with cancer were diagnosed at a later stage more frequently than the other groups. However, statistical analysis adjusting for cancer stage showed that later diagnoses did not fully explain the disparities in survival. The researchers say the study highlights the need for potentially life-saving policy interventions—both within and outside of prisons.
“It’s incredibly important for health care systems, including Smilow Cancer Hospital, to think about the care that’s provided to those that are incarcerated or immediately post-release as a potential intervention point for tackling persistent racial and socioeconomic disparities in cancer care,” says Wang. Many of the incarcerated patients she worked with, for example, are taken to cancer centers in shackles for chemotherapy. “You’re likely to start losing trust in the health care system if those are the policies that are in place to get cancer care.”
Working toward achieving health equity
Since coming home three years ago, Cruz has been focusing on his health and spending time with his daughter and six-year-old grandson. “I got out when he was three years old, and I’m hoping to be around for the next forty,” he laughs. At first after being released, he struggled to feel heard by his provider, but now, he says, he sees an “amazing” oncologist in Bridgeport.
Cruz describes himself as someone who does not like to do a lot of talking, but an oncologist who treated him while he was incarcerated encouraged him to share his story. He was further encouraged by Tino Negron, a research aide at the SEICHE Center. “Sometimes I shut down, but by the grace of God, I have more support now being home with my family, he says. “But it’s been a journey.”
For many other recently released individuals, as highlighted by Wang and Gross’s work, accessing care and support is a challenge. The team says the U.S. can reach health equity, however, through striving to remove systemic barriers to care. Within prisons, this means improving access to primary care services and adhering to cancer screening guidelines so that diagnoses are not unnecessarily delayed. But work needs to be done outside the prison’s walls, too. Achieving cancer care equity will also require addressing obstacles to receiving care in at-risk communities, ensuring recently released individuals are following up with their medical care, and integrating cancer prevention into programs that are focused primarily on the health needs of people who return from correctional facility, like Transitions Clinic programs in New Haven.
“Achieving health equity is possible, but it needs to be a central goal of all that we do as a health care system,” says Gross. “It won’t happen by accident—a rising tide does not lift all boats. As a society, we need to stop torpedoing some boats before they have a chance to sail.”
More information:
Oluwadamilola T. Oladeru et al, Incarceration status and cancer mortality: A population-based study, PLOS ONE (2022). DOI: 10.1371/journal.pone.0274703
Journal information:
PLoS ONE
Source: Read Full Article